")
Healthcare revenue rarely disappears because the care was poor. It goes uncollected because the money owed remains in accounts receivable for too long.
More of that money now sits with patients. The KFF’s 2025 Employer Health Benefits Survey mentions that the average single-coverage deductible reached $1,886. It shifts a larger share of every bill onto patients, who pay more slowly than insurers do. That is recoverable revenue, aging past the point where collecting it is easy.
Strong healthcare accounts receivable management is what keeps that money moving. This guide explains what AR management is and why healthcare AR ages faster than in other industries. It also covers the metrics that matter and how to recover patient and payer balances without straining the relationship.
Contents
- 1 What is Healthcare Accounts Receivable Management?
- 2 Why Healthcare AR Ages Faster Than Other Industries
- 3 The AR Metrics That Matter, And the Benchmarks
- 4 Best Practices to Manage Healthcare AR
- 5 Managing Patient AR Specifically
- 6 Compliance in Healthcare AR
- 7 In-House vs Outsourced AR Management
- 8 How First Credit Services Supports Healthcare AR
- 9 Turn Aging AR Back into Cash Flow
- 10 FAQs
- 10.1 1. What are good days in AR for a healthcare provider?
- 10.2 2. What is the difference between AR management and medical billing?
- 10.3 3. What causes high accounts receivable in healthcare?
- 10.4 4. How can hospitals reduce AR aging?
- 10.5 5. Should healthcare providers outsource AR management?
- 10.6 6. Is patient AR different from insurance AR?
What is Healthcare Accounts Receivable Management?
Healthcare accounts receivable management is the process of tracking and resolving all balances owed to a provider, from claim submission through the last dollar paid. It covers both the payer side (insurance claims and reimbursement) and the patient side (deductibles, copays, and coinsurance).
It is often confused with related revenue cycle functions, but each serves a different purpose:
- Medical billing: The front end of the process, including coding patient encounters, submitting clean claims, and posting payments.
- Medical accounts receivable management: The follow-up stage, where unpaid or denied balances are worked until they are resolved.
- Revenue cycle management (RCM): The complete financial process, from patient registration and insurance verification to final payment and reporting.
Put simply, medical billing creates the receivable, while AR management turns it into cash. Healthcare receivables management applies this process across both payer and patient balances, whether for hospitals, physician groups, or other healthcare providers.
Why Healthcare AR Ages Faster Than Other Industries
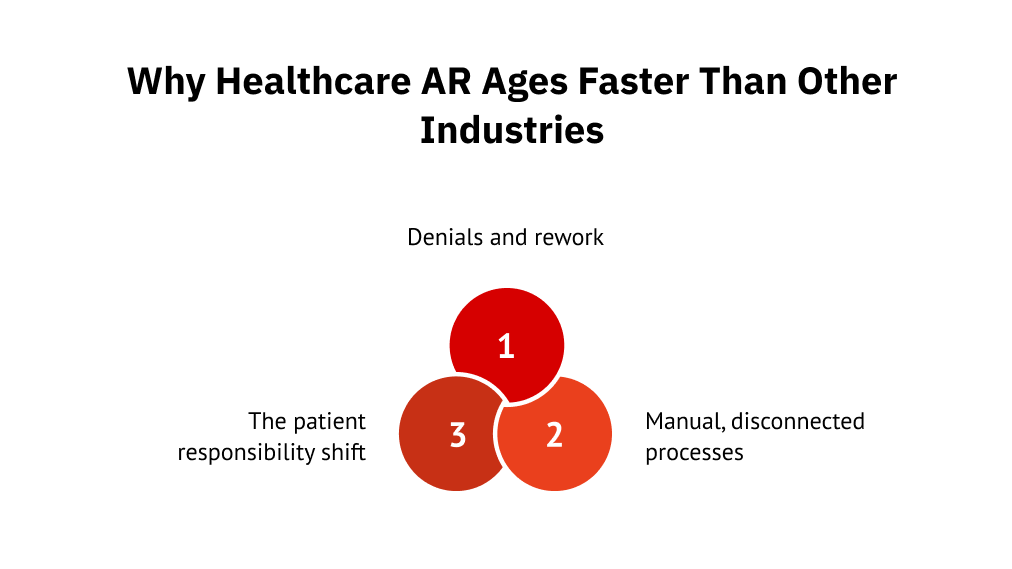
Every industry has slow payers. Healthcare adds a structural problem: a single balance often has two payers (insurer and patient), two clocks, and two failure points. When either side stalls, the balance ages. Three forces make it worse in the following ways:
1. The patient responsibility shift
A growing share of every bill now falls on the patient rather than the payer. High-deductible health plans have made patient balances one of the fastest-growing parts of provider revenue. And that share collects differently than insurance.
That shows up in behavior: patients pay less of what they owe as the balance grows.
That shows up in behavior: patients pay less of what they owe as the balance grows. In the Federal Reserve’s 2024 SHED survey, 37% of adults could not cover an unexpected $400 expense with cash. So larger balances get paid in pieces or stall, the same dollar sits longer, and the biggest patient balances, the ones worth chasing, are the hardest to collect.
2. Denials and rework
Denied claims are one of the biggest reasons healthcare AR remains unpaid for longer. Every denial delays reimbursement and requires additional time and effort to investigate, correct, and resubmit the claim.
Without a structured denial management process, claims can sit untouched, miss filing deadlines, or require repeated rework. The longer they remain unresolved, the lower the chances of recovering the full payment.
3. Manual, disconnected processes
When aging reports live in spreadsheets and payer portals sit behind separate logins, it’s hard to see which accounts are aging or who owns the next step. Balances slip past filing deadlines, follow-ups are duplicated or missed, and collection costs rise with every manual touch. The work isn’t the problem, but the lack of visibility is.
The AR Metrics That Matter, And the Benchmarks
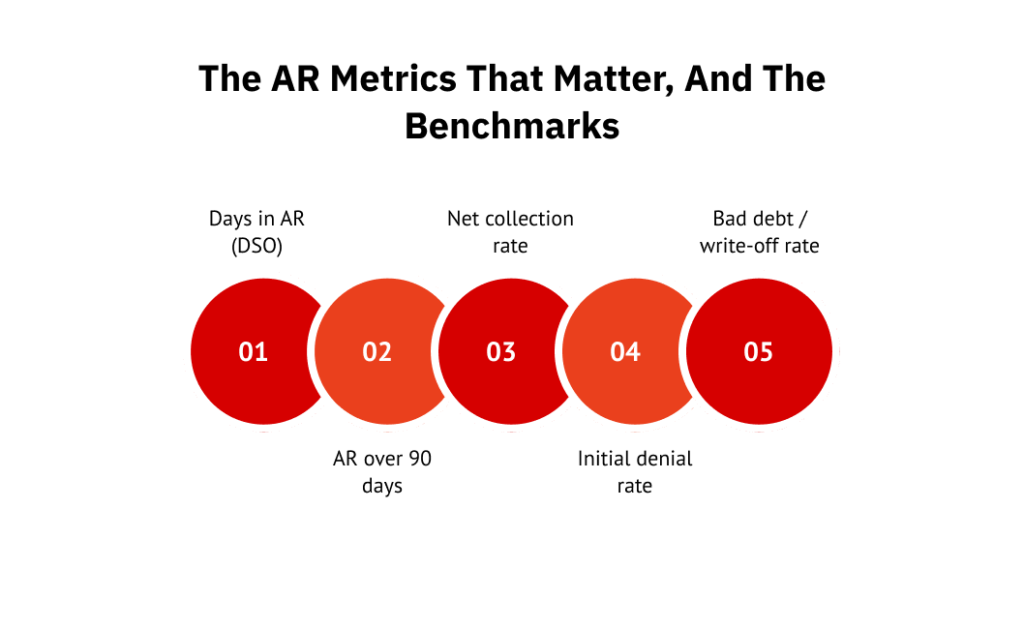
You cannot manage healthcare AR; you cannot measure. A handful of metrics tell you whether cash is moving or quietly backing up. Track these together, since one metric can look fine while another hides the problem.
| Metric | What it measures | Common target |
| Days in AR (DSO) | How long, on average, a dollar waits to be collected | Under 40 to 50 days; 30 to 35 is high-performing |
| AR over 90 days | Share of total AR that has aged past 90 days | Historically 20% or less; many systems now sit well above |
| Net collection rate | Share of allowed, collectible revenue actually collected | 95% or higher |
| Initial denial rate | Share of claims denied on first submission | Single digits; under 5% is strong |
| Bad debt / write-off rate | Revenue written off as uncollectible | As low as the payer and patient mix allows |
Two of these deserve a closer look, because they tend to move first when AR is in trouble.
1. Days in AR and DSO
Days in AR tells you how long the average dollar waits before it is collected. The math is simple enough to run yourself: total AR divided by average daily charges. If your total AR is $3 million and you bill $100,000 a day on average, you are sitting at 30 days in AR.
The common operating target is under 40 to 50 days, with 30 to 35 days considered high-performing. The number matters less than its direction. A figure climbing month over month warns that claims are stalling or patient balances are piling up, well before it shows in the cash report. That is why DSO reduction is worth treating as a standing goal.
2. AR aging buckets
Splitting AR into 0-30, 31-60, 61-90, and 90-plus day buckets shows where the money is stuck. The 90-plus bucket is the one to watch, because collectability drops sharply once a balance crosses it.
By then, contact information has gone stale, filing windows are closing, patient recall has faded, and newer balances compete for the team’s attention. When your 90-plus bucket climbs past the low-teens, that is the signal to act, not the time to write it off.
Best Practices to Manage Healthcare AR
Good healthcare AR management is mostly a set of habits done consistently, not a single fix. The practices below work because they shorten the time a balance spends aging and cut the number of balances that need heavy recovery later.
- Verify eligibility and benefits before the visit, so claims do not bounce due to coverage errors.
- Collect at the point of service, when the patient is present, and the balance is fresh.
- File clean claims the first time. Front-end accuracy is cheaper than back-end appeals.
- Work aging reports on a fixed weekly cadence, not whenever someone has time.
- Run a structured denial follow-up loop with owners and deadlines for each denial reason.
- Offer flexible payment options, including plans, before a patient feels cornered.
- Automate reminders across channels so follow-up does not depend on staff bandwidth.
- Escalate aged balances on a written policy, so nothing sits in limbo by default.
Prioritize the work
Not every balance deserves equal attention. Work accounts by dollar value and age, not on a first-in, first-out basis. A handful of high-dollar denials nearing their appeal deadline will return more than a stack of small, fresh balances. Let value and urgency, not arrival order, set the queue.
| Pro Tip: Phone-only follow-up leaves money on the table. Layering multichannel patient outreach across SMS, email, and a self-service portal reaches patients on the channel they actually use and lifts response rates over calling alone. |
Managing Patient AR Specifically
Patient AR does not behave like insurance AR, and patient AR management that copies the insurance playbook is why so much of it ages. The balance is smaller, the payer is a person, and the reasons it goes unpaid are mostly about clarity and timing, not refusal.
Why do patient balances behave differently
Patients rarely delay because they refuse to pay. They delay because they are confused by the bill, surprised by the amount, or unsure what insurance already covers. A statement that arrives weeks after the visit widens that gap, since the care is no longer fresh and the charge feels disconnected from it.
That lag is the quiet killer of patient AR. The longer the wait between service and a clear final statement, the weaker the recall and the lower the odds of payment.
Communication as a recovery lever
Because the problem is mostly clarity, communication is the lever that moves patient balances. Clear, itemized statements, upfront cost estimates, and payment plans recover more than firmer letters do, without straining the relationship.
The mechanics matter as much as the message. Self-service portals and reminders via SMS, email, and web let patients view their balances and pay on their own time, which improves completion rates. A $480 balance split into four monthly payments through a link in a text resolves far more reliably than the same balance sitting on a paper statement waiting for a phone call.
Compliance in Healthcare AR
Healthcare AR sits inside two regulatory frameworks at once, which is what makes it different from collecting any other receivable. Getting the recovery right and the compliance wrong is still getting it wrong.
The regulations that apply
HIPAA governs how patient data is handled, stored, and shared at every step of AR work. It also includes who can view a balance and how that information can be communicated. The Fair Debt Collection Practices Act governs collection conduct. State rules add additional restrictions, while the TCPA shapes how and when organizations can send texts or make calls.
These are not edge cases in healthcare AR. Patient balances carry protected health information by default. Thus, a sloppy reminder or a misdirected statement is both a recovery miss and a potential breach.
What compliant AR looks like in practice
Compliance in AR is mostly documentation and discipline. In practice, that means documented processes and audit trails that hold up under review, call monitoring, and clear records of every patient interaction.
It also means proper consent capture before SMS outreach, honored opt-outs, and controlled contact frequency. When the rules are built into the workflow, compliant outreach and faster recovery no longer compete.
In-House vs Outsourced AR Management
At some volume, the question stops being how to work AR better and becomes who should work it. Most healthcare organizations end up with a hybrid, keeping some AR in-house and sending the rest to a partner. The table below frames the tradeoff.
| Factor | In-house | Outsourced parter |
| Cost | Fixed staffing, harder to flex | Variable, often contingency-based |
| Scale | Capped by headcount | Absorbs volume spikes |
| Denial expertise | Depends on internal depth | Specialized, payer-specific |
| Compliance | You own all of it | Shared, with vendor controls |
| Technology | You buy and run it | Included and managed |
| Speed | Limited by bandwidth | Built for consistent follow-up |
Signs it is time to get outside help
The numbers usually say it first. AR aging past 90 days, a DSO that stays above benchmark, or a denial rate that keeps creeping up all signals that the internal team is past capacity.
The softer signs matter too, such as:
- Staffing gaps that never close
- A backlog that the team cannot clear
- Aged accounts are touched once and abandoned
When the queue grows faster than it shrinks, more effort will not fix it.
What to look for in a partner
The right partner does more than make calls. Ideally, you should look for:
- Healthcare-specific AR experience, not general collections
- Real compliance credentials (HIPAA, PCI, and SOC 2 at a minimum).
Also, evaluate how they engage patients and share results. Look for omnichannel outreach instead of phone-only collections, transparent reporting with real-time visibility, and a recovery approach that protects your brand. The right partner recovers outstanding balances while preserving patient trust and encouraging future care.
How First Credit Services Supports Healthcare AR
First Credit Services works across the full revenue cycle as a revenue recovery and patient engagement partner, not a late-stage collector. That distinction matters in healthcare, where the patient on the other end of a balance is also the patient you want back for the next visit.
Its digital, omnichannel outreach is powered by Unified Consumer Engagement Platform (UCEP), which integrates with your existing billing system instead of replacing it. Here’s what it offers:
1. Patient-balance recovery without brand damage
For patient balances, FCS uses first-party collections. Thus, patients experience reminders and statements as part of your organization, not as a third-party handoff. The experience stays under your brand from the first message to the final payment.
That outreach pairs with self-service payment options and flexible plans, the same mechanics that lift patient AR recovery. A patient can open a personalized link, see the balance, and set up a plan without calling anyone, resolving more balances while keeping the relationship intact.
2. Extended support and reporting
When internal teams are stretched, FCS’s extended business office (EBO) services provide ongoing AR follow-up that scales with volume instead of headcount. They also offer broader patient engagement and back-office support for work that extends beyond collections. The outreach stays consistent across channels via the omnichannel model.
Clients get customizable dashboards for real visibility into recovery, by aging buckets and channels, without managing the platform themselves.
Turn Aging AR Back into Cash Flow
Healthcare AR is recoverable revenue waiting on the right process. Watch the 90-plus bucket, fix denials at the source rather than reworking them later, and align patient outreach with how patients actually want to pay. Do all three consistently, and you will reduce days in AR, improve cash flow, and minimize avoidable write-offs.
Want to recover more without compromising the patient experience? Talk to FCS about turning your aging report back into working capital.
FAQs
1. What are good days in AR for a healthcare provider?
Most providers aim for under 40 to 50 days in AR, with 30 to 35 days considered high-performing. The trend matters more than the number, since a figure climbing month over month signals claims are stalling or balances piling up.
2. What is the difference between AR management and medical billing?
Medical billing creates receivables by coding and submitting the claim. AR management is the follow-up work that turns it into cash when it does not resolve on the first pass, including denial follow-up and patient balance recovery.
3. What causes high accounts receivable in healthcare?
Main causes include unworked claim denials, the growing share of patient responsibility under high-deductible health plans, and slow patient payments. Manual processes also make it difficult to identify aging accounts and determine who is responsible for the next follow-up.
4. How can hospitals reduce AR aging?
Hospitals reduce AR aging by verifying eligibility upfront, filing clean claims, reviewing aging reports weekly, running structured denial follow-up, and offering flexible, multichannel payment options so patient balances are resolved before they reach 90 days.
5. Should healthcare providers outsource AR management?
Outsourcing makes sense when AR consistently ages past 90 days, DSO stays above benchmark, or staffing cannot clear the backlog. Many providers keep early follow-up in-house and outsource aged or high-volume balances to a specialist.
6. Is patient AR different from insurance AR?
Yes. Insurance AR turns on clean claims and denial follow-up. Patient AR prioritizes clarity and convenience, since patients usually delay due to confusion or timing rather than refusal. Clear statements, estimates, and easy payment options help recover it faster.